Media
Vaccines: safe or sorry?

In the week before Christmas of 2014, the Disneyland theme park saw what its officials least expected. A child, suffering from measles, came to the park. This child exposed many other customers and staff. As of 24 January 2015, California health officials counted 85 active measles cases. The media seemed to go into frenzy overnight. Breathless reports screamed, “We had eradicated measles in 2001, and now see what!” Reporters uniformly concluded: vaccines against measles had contained and even eliminated the disease in the United States in 2001. Then, foolish parents rebelled against vaccines and refused to let their children take them. With the alleged results they scream about now. But are they telling the truth? Or has the debate on vaccines taken a one-sided turn? And does that threaten not only individual liberty, but also free scientific inquiry and even the health of the public?
The case for vaccines
Fox News Channel and nearly every other media organ all make the case for vaccines. Vaccines confer active acquired immunity to a disease. So goes the theory. Challenge the patient with a virus (the usual sort of agent involved) identical or similar to one that causes human disease. Let the body raise an immune response to it. Now the patient can fight the “wild type” and so avoid falling sick from that type. Proponents of vaccines point to several diseases that once killed many and now happen rarely: diphtheria, pertussis (“whooping cough”), tetanus, poliomyelitis, smallpox (variola), chicken pox (varicella), and the Big Three: measles, mumps, and rubella (the German measles).
To make the case solid, doctors must convince themselves, their patients, and the public of one thing: will the patient do better with their treatment than without it? Every doctor (including your correspondent, who has a medical degree) learns this First Rule of Medicine: do no harm. That principle informs the oath Hippocrates of Cos made his students swear by, more than two thousand years ago. And to convince people to take (or make others take) vaccines, doctors must answer these questions:
- What chance does the patient take on getting the wild-type disease without taking the vaccine?
- How bad will the wild-type disease affect him if he catches it?
- What chance does the patient take on either getting the disease, or suffering some other problem (doctors call this a complication), if he does take the vaccine?
- How badly will he suffer in that event?
At least, those who make vaccines, and want to force everyone to take them, think those four questions “cover” the patient’s concerns. And on Questions 1 and 2 the case seems compelling. The “Iron Lung” (negative pressure ventilation) seems a distant memory today. Rubella, more than any other virus, often injured the developing brains of unborn children whose mothers came in contact with active cases. Results varied from congenital deafness to severe mental impairment. Anyone would want to cut, and to zero if they could, anyone’s chances of suffering that sort of result.
But in 1993, to your correspondent’s personal knowledge, the Centers for Disease Control goofed, and goofed badly, on preparing the influenza vaccine. Your correspondent took that vaccine, traveled to Orlando, Fla., came back, and came down with the ‘flu anyway. Even today the CDC cannot guarantee their vaccines will always stop you from getting the ‘flu. By many accounts, this year’s ‘flu vaccine has the worst numbers in decades for people taking the vaccines and getting the ‘flu anyway.
In fact, those four questions assume, without warrant, one hundred percent effectiveness in the vaccines, and no alternatives other than social isolation to stop the spread of the wild type. So now we must ask ourselves two more questions:
- What chance does the patient taking the vaccine, run of getting the wild type anyway?
- What else can the patient do to ward off the wild type, or make it less severe?
But the media won’t ask those questions. And they mock those who do.
The case against vaccines
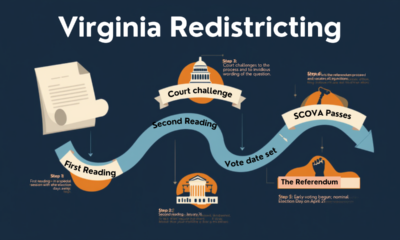
Measles incidents in the United States, 1950-2001. Source: CDC
Those who push vaccines hardest have harmed their credibility already. Who says the CDC or anyone else eradicated measles in the United States? Even the CDC does not say that. They had a plan to eradicate measles. But simple Internet engine searches fail to disclose their triumphant report they did so eradicate measles. (One such report might have existed. But the CDC seems to have taken it down. Why?)
More to the point, authorities never seem to have considered the effects of giving so many vaccines, not merely one at a time, but several, with little time between them. This could overwhelm the immune system. The vaccine then would not help the patient at all. Or worse: all those vaccines could provoke the immune system to attack the patient’s own body. Or the vaccine strain could affect the patient in ways no one has ever studied, or had time to study.
In 1998, Andrew J. Wakefield, M.D., published a study in Lancet alleging patients who took a common combination vaccine, the MMR (measles, mumps, rubella) also took a chance on developing a pervasive developmental disorder, either the classic “autism” (the infantile variety) or the childhood-onset variety. Six years later, Mr. Brian Deer, ostensibly writing for The Times (London, England, UK), began his own “investigation” of Wakefield. His conclusion: Wakefield published a bogus report. Worse, a number of lawyers paid Dr. Wakefield to write a critical report. Those lawyers, said Deer, wanted evidence to sue the drug companies that made this and other vaccines.
But Joseph R. Mercola, D.O., in 2006 found reason to suspect Deer and others of lying outright. He cited this piece by J. B. Handley. Handley disclosed several inconvenient facts about Brian Deer. Deer pretended to be in the employ of the Times. He wasn’t. Moreover, Dr. Wakefield did not even talk to any lawyers until he had already done a lot of his research. He didn’t front for any lawyers. But Mr. Deer took money from drug companies. Worse than that, Mr. Deer filed the first complaint against Wakefield! Nor does the tale of corruption end with Mr. Deer. The CEO of Lancet joined the Board of Directors of Glaxo SmithKline shortly before Deer’s first damning article came out in the Times.
What prompted Dr. Mercola to write about the Wakefield-Deer kerfuffle? Someone else already had reason to believe Dr. Wakefield was right.
Readers can look at Dr. Mercola’s articles on measles here.
Today, even the Fox News Channel anchors talk of “study after study” invalidating Dr. Wakefield’s claims. Lancet published this one within a year of Dr. Wakefield’s own study. But how can we believe this, if the CEO of Lancet won a place on the Board of Directors of Glaxo SmithKline after that? More to the point, has any independent researcher, concerned only with medical truth, looked at the data honestly?
Drug companies do fund research studies. But they usually fund studies that will point to a drug they’re developing, as a “clinical solution.” Have we independent studies, by those interested only in “looking out for the folks,” as Bill O’Reilly loves to say?
Regulators get it wrong
[ezadsense midpost]
Furthermore: regulatory agencies have gotten it wrong, even horribly so, before. Two such cases make this point. First is Baycol (cerivastatin/Bayer). Bayer AG withdrew this “statin” drug from the market in 2001. The FDA had approved it in 1997. After that, thirty-one patients took it, developed rhabdomyolysis (in which the “striated” or “rod-containing” muscles of the skeleton broke down), and died.
Next: Vioxx (rofecoxib/Merck, Sharpe and Dohme). Does anyone still remember Dorothy Hamill endorsing that drug, and taking a turn on the ice rink before two adoring little “next-generation figure skaters,” and talking about how Vioxx let her skate again? Merck withdrew it in 2004. Why? Because too many patients took it, suffered heart attacks and/or strokes, and died.
Those two cases alone provoked a debate on how many drugs had the FDA approved, when it shouldn’t have. Today the law firm of Pulaski and Middleman (the 1-800-BAD-DRUG firm) has made a reputation for helping patients suffering from adverse reactions from all kinds of drugs. They have cases pending for nineteen drugs and drug classes today. Among them: Lipitor (atorvastatin/Pfizer), a close cousin to Baycol. And Fosamax (alendronate/Merck), a drug doctors use to treat osteoporosis. Among the side effects no one caught until too late: idiopathic thrombocytopenic purpura. Patients take this, and their bodies start attacking their blood platelets. They then break out in one continuous bruise all over their bodies!
(This firm has not yet responded to a request for comment on the current controversy on vaccines, or a question of whether they have vaccine cases pending.)
The case against Andrew Wakefield persists on the Web. But those making that case, rely on unreliable witnesses. More ironically still: some of the same people who sullied Dr. Wakefield’s reputation, earlier decried the link between pharmaceutical development and basic and clinical research. How quickly they decided they could trust drug companies, when they seemed to tell them what they wanted to hear. So they could say things like this, without a trace of irony:
Sometimes the health and well-being of the many DOES trump the rights of the few.
Except that, beyond the question of individual liberty, the evidence is inconclusive, and has its basis not only in fraud but in a travesty of justice.
For further information, see the National Vaccine Information Center.
[ezadsense leadout]


Terry A. Hurlbut has been a student of politics, philosophy, and science for more than 35 years. He is a graduate of Yale College and has served as a physician-level laboratory administrator in a 250-bed community hospital. He also is a serious student of the Bible, is conversant in its two primary original languages, and has followed the creation-science movement closely since 1993.








-

 Civilization4 days ago
Civilization4 days agoWinning in Iran Requires More Than Military Success
-

 Civilization4 days ago
Civilization4 days agoEpic Fury as It Is: A Look Inside
-

 Guest Columns4 days ago
Guest Columns4 days agoWaste of the Day: $34 Billion In Secretive Military Funding
-

 Education3 days ago
Education3 days agoWaste of the Day: School Officials Claim Safari Was “Professional Development”
-

 Executive3 days ago
Executive3 days agoHell No, We Won’t Go!: A Florida Man’s Response to NY’s Gov. Hochul
-

 Executive3 days ago
Executive3 days agoWaste of the Day: Throwback Thursday – Crash Landing for NASA Video Game
-

 Civilization2 days ago
Civilization2 days agoReclaiming the Lunar High Ground
-

 Executive1 day ago
Executive1 day agoWaste of the Day: Alabama Hired Lawyer for Lawsuits He Caused
I don’t know what your ‘simple internet searches’ involved, but they seem to have missed a _lot_:
link to jid.oxfordjournals.org “Molecular data support the proposition that endemic transmission of measles has been interrupted in the United States.” (March, 2000)
link to cdc.gov “In 2000, the US declared that measles was eliminated from the country”
link to jid.oxfordjournals.org “The refined strategies of the third ongoing measles-elimination effort have achieved success. Measles is no longer endemic in the United States.” (2004)
link to ncbi.nlm.nih.gov “The United States documented the elimination of endemic measles in 2000 and of endemic rubella and CRS in 2004. In December 2011, the Centers for Disease Control and Prevention convened an external expert panel to review the evidence and determine whether elimination of endemic measles, rubella, and CRS had been sustained…The external expert panel concluded that the elimination of endemic measles, rubella, and CRS from the United States was sustained through 2011.” (2014)
Does Wakefield’s conflict of interest w/r/t his own measles vaccine weigh as heavily on your mind as your perceived conflict of interest of the CEO of _Lancet_? What about the BMJ or the British General Medical Counsil?
“Except that, beyond the question of individual liberty, the evidence is inconclusive, and has its basis not only in fraud but in a travesty of justice.” It’s not clear what evidence you’re talking about here – evidence against the effectiveness or safety of vaccines in general? Wakefield’s results? Wakefield’s personal misconduct? – but it’s clear that Wakefield’s study has been retracted (link to thelancet.com), that Wakefield’s research was found to be fraudulent (link to bmj.com) and that Wakefield was stripped of his medical license in the UK for multiple ethics violations related to his 1998 study (link to briandeer.com). Also, it’s clear that subsequent studies have not shown any association between measles vaccination and autism as Wakefield had claimed (link to ncbi.nlm.nih.gov) or (link to cdc.gov).
First: Wakefield never had a trial in a court of law on the question of any conflict of interest nor even on any question of fraud, scientific or otherwise. Never once did he have his day in a forum having rigorous rules of evidence. Instead he faced a kangaroo court. Hence my opinion: he did not get a fair trial. He did not get a trial at all. My opinion, were I an appellate judge, would be: remand for a new trial. A proper trial.
Second: his judges, such as they were, were corrupt. They took drug-company money. One of them, the CEO of Lancet, took an appointment to the Board of Directors of Glaxo SmithKline. Did you not read my statement to that very effect?
Third: what threat does a non-immunize host pose for an immunized host? Can an immunized host acquire an infection from a non-immunized host who acquires an infection himself? (And why is it that anyone, having taken an immunization, must avoid contact with immunocompromised persons for a specified time? How does that square with “minimizing risk to the population”?)
If an “immunized” host acquires an infection, who really is at fault? The non-immunized host? Or the maker of the immunizing preparation, whose preparation turned out to be less than fully effective?
Seriously? Aren’t you a doctor? I’m not even vaguely in the medical world and I know the answer to most of these.
>what threat does a non-immunize host pose for an immunized host?
None, assuming the vaccination worked on them. However, there are plenty of people who are unable to receive the vaccination, e.g. the very young, old, immunocomprimized, etc. They pose a threat to any of those people.
>Can an immunized host acquire an infection from a non-immunized host who acquires an infection himself?
No, assuming the vaccine worked.
>And why is it that anyone, having taken an immunization, must avoid contact with immunocompromised persons for a specified time? How does that square with “minimizing risk to the population”?
While the risk is low, there is a non-zero chance they could spread it to an immunocomprimised person while their immune system is fighting off the vaccine. It’s the same reason you shouldn’t give that same person the vaccine.
>If an “immunized” host acquires an infection, who really is at fault? The non-immunized host? Or the maker of the immunizing preparation, whose preparation turned out to be less than fully effective?
The non-immunized host, no question. While you were practicing (you’re not currently practicing medicine are you? I seriously hope not with this kind of irresponsible medical advice), did you only prescribe medicine that had 100% effectiveness? Not 99%, not 99.99999999%, literally zero percent chance it won’t work?
You’re aware of the concept of herd immunity, right? I assume that would have been covered at medical school.
You have just negated any kind of legal case anyone can make in a free society.
“Herd immunity” is an inherently offensive concept to any free human being. It connotes literally herding people like cattle. Is that what you really want to stand on and for?
The British GMC spent two and a half years investigating Wakefield’s conduct surrounding his 1998 Lancet study. The five member board solicited testimony from >30 witnesses as well as Wakefield and his co-authors. The council’s burden of proof was ‘beyond reasonable doubt’, which matches the criminal burden of proof rather than the looser civil burden of proof. Wakefield was represented by legal counsel, as was the ‘prosecution’. The GMC found that Wakefield:
Failed to disclose potential conflicts of interest in his research application to the Ethics Committee (prior involvement in MMR lawsuit, anti-MMR work for a legal group, work on a novel measles vaccine).
Performed invasive procedures (colonoscopies and biopsies) on multiple patients for research purposes without Ethics Committee approval.
Ordered lumbar punctures on multiple patients for research purposes contrary to the clinical interest of the patients AND in violation of his terms of employment AND contrary to the research protocol he had presented to the Ethics Committee.
Ordered tests for patients for research purposes, claiming diagnoses that the patients did not have.
Did not disclose conflicts of interest to Lancet, or reveal that the patients described in the Lancet paper had been admitted expressly for research purposes and were effectively cherry-picked by Wakefield and his group. The GMC found this dishonest, irresponsible, and misleading.
Was irresponsible, misleading, and violated the duty of a main author in his description of the patient population in the Lancet paper. Further, when challenged as to the possibility of selection bias in the study patients, gave dishonest, irresponsible responses.
Presented dishonest, irresponsible, etc., statements in scientific meetings related to the Lancet study.
Administered experimental therapy to a patient without recording it in the patient’s medical record, contrary to the interest of the patient.
DREW BLOOD SAMPLES FROM CHILDREN AT A BIRTHDAY PARTY FOR RESEARCH PURPOSES AND COMPENSATED THEM WITH MONEY AFTERWARD without ethics committee approval, in abuse of position of trust as a medical practitioner.
The GMC held these behaviors to represent serious professional misconduct and therefore stripped Wakefield of his medical license in 2010.
Frankly the guy is lucky he _didn’t_ have a trial in a court of law, and that the only sanction he faced was the loss of his license and the retraction of his paper. I’m frankly astounded that you would support this guy when he was performing research on patients before he had ethics committee approval. How do you justify patients being studied in 1996 when approval for the ‘project’ didn’t come through until 1997? Haven’t you heard of IRB approval? Do you think it’s appropriate to ask children to give blood samples at a birthday party for research purposes?
It was _after_ the GMC report that the Lancet retracted the paper. The GMC report did not even address other issues that came to light later: that Wakefield falsified clinical histories and neuropsych diagnoses for some of the study patients, or that intestinal biopsy specimens read as normal were reported as showing colitis in the Lancet paper. Do you think that’s how research should be done?
The non-immunized host presents a threat to the immunized host because vaccination is not a magic bullet that renders 100% immunity forever. Some vaccines are more effective and longer-lasting than others, which is why you need a tetanus booster every few years but only one course of polio vaccinations. Even in the case of vaccines that are generally quite effective, there are individuals who for whatever reason do not mount an effective response to the vaccine – and in the absence of universal titers post-vaccination, they would have no way of knowing this. I myself have can only boast weak titers against varicella zoster, despite having an occult case of chicken pox in childhood AND having been vaccinated several times. Immunized people get cancer or develop autoimmune disorders or get AIDS too, and lose their ability to fight off infection despite their earlier immunization.
An immunized host does not present the same degree of threat to another immunized host; they represent a _decreased_ threat (albeit typically nonzero) to each other. An unvaccinated host presents a asymmetric threat to a vaccinated host, benefiting from the reduced risk that the vaccinated person presents back. Would you, personally, be happier sharing a long bus ride through Lagos with a random group of people who had been vaccinated for measles and pertussis and chicken pox, or a random group who had not been so vaccinated?
So yes, an immunized host can sometimes acquire an infection from an infected non-immunized host. But of course you knew that, based on your 1993 flu experience. Immunization is a numbers game; it aims to reduce the likelihood of transmission of disease from one person to the next to the degree that each infected patient will on average infect less than one other person, thus preventing the spread of the illness through the population. Even if vaccination was 100% effective for a given strain, the unvaccinated population can serve as a reservoir for the disease and thus a potential source for new mutant versions of a disease which are not covered by the vaccination. Think of all those birds and pigs mingling on farms in Asia that churn out new strains of influenza every year. Also, not everyone can be vaccinated for every condition: infants, the immunocompromised, persons with particular allergies, etc. _Those_ groups rely on herd immunity, which requires a high enough penetrance of immunization in the population to interrupt transmission.
‘Anyone taking an immunization..must avoid contact with immunocompromised persons’ – what bull is this? There are SOME live attenuated vaccines (MMR, Rotavirus, Chicken Pox, Typhoid, oral Polio, nasal Influenza) that cannot be used by immunocompromised patients, or by those who will have contact with such persons, because the immunizing agent is a weakened form of the disease organism, which normally presents no challenge to a healthy immune system but can overwhelm a disabled one. The tradeoff is that the attenuated vaccines produce stronger, longer lasting immunity. Others (injectable Polio or Influenza, Pertussis, Tetanus, Hepatitis B, HPV, Typhoid, Plague, Hib, Meningococcal, Pneumovax, Diphtheria) used killed viruses or bacteria or toxoids and can’t cause illness in immunocompromised hosts. Attenuated vaccines still minimize risk to the population – why wouldn’t they?
Where do we see outbreaks of vaccine-preventable infectious disease in the US nowadays? Do clusters crop up in areas where there are lots of immunized people and herd immunity provides protection for those individuals who _can’t_ get vaccinated, or who were vaccinated but either didn’t respond or have decreased immune function overall? Hint: no – they occur in areas where immunization rates are lower, and there are enough susceptible individuals to keep outbreaks going. Who’s more at fault – the person who attempts to minimize risk but may not be 100% successful, or the person who makes no effort to reduce risk at all?
Every one of the charges against Dr. Wakefield you mention, is in dispute. You might consider the dispute settled. I do not.
The rest of the above screed now turns into an argument for turning the entire society into a major quarantine ward.
This illustrates a principle I have long observed: I have never seen a bigger wuss than a dedicated leftist voter or politician.
Add to it: leftists once supported Dr. Wakefield completely. They turned against him only when they realized the vaccine regime was a means, not primarily to enrich “evil private companies,” but to provide a measure of total government ownership and control over the lives of its
citizenssubjects.Herd immunity is offensive? Is that a joke?
The principle is mathematically sound: the more immune people there are in a population, the less likely it is that a sick person will come in contact with a non-immune person and be able to infect them. The fraction of the population that must be immune in order to prevent spread of a disease varies depending on just how infectious the disease is.
Think of it as ‘rugged individualist immunity’ if your sensibilities are so fragile.
Mathematically sound it might be. But consistent with individual liberty and human dignity it most certainly is not. Mathematical soundness must fall before the concept of individual liberty and self-fortification, whether in the context of infectious diseases or in self-defense against crime.
The concepts “herd immunity” and “gun control” proceed from the same wussified ideological source.
Should food service workers -have- to wash their hands before they return to work after using the bathroom? Let’s assume that the boss doesn’t care, because the boss has closely held beliefs about limitations on personal freedom. Should there be a law about how long a restaurant can leave potato salad sitting out on the counter without refrigeration before serving it?
Does a person with influenza have any obligation to stay home from work or school when they are sick, or to cover their coughs and sneezes when they are out and about?
Should driving drunk be a criminal offense, especially in the absence of damages to persons or property?
I would imagine that in a libertarian utopia a sick person would rationally chose to go to work and continue to earn wages rather than skip a few days. The health of the other employees of the company or in the general community is not his responsibility. Perhaps the employer would object, but what right would the employer have to demand that the sick person stay home?
Food service is something you get paid to do.
You want to know how much an ordinary civilian gets paid to have this challenge done to his body?
Zero. Big fat round nothing.
Kindly repair your argument.
Influenza is the Favorite Malingerer’s Ailment, as bosses everywhere almost universally declare.
Driving is, of course, a privilege, not a right. The government, to my regret, owns all the streets and roads. Therefore the government sets the rules of those roads. A thing I seek to change. Then, of course, I doubt any owner/operator of any road would care to let anyone drive on it if he is less than able to control his vehicle.
All people have the right to stay healthy and be free from those that would place that health in danger; no one has the right to endanger others.
Taking care to not bring harm to those that can not protect themselves (elderly, young, allergic, immunocompromised) should be a personal goal for every person.
If one exercises their freedom to not be vaccinated, then they lose the privilege to go or work in places that put them in close proximity with others whom through no fault of their own didn’t have the option e.g. schools, hospital & food service workers.
By all means, exercise your right not to immunize. Because stoking your ego, and affirming your privilege is the most important thing to do. But that’s you right.
However, with rights come responsibilities. And if you – through your own choice – are not safe to be in a crowd, then you cannot complain if steps are taken to remove you from all public places – shops, offices, libraries, parks, stadiums, etc, until such time as your choice does not pose a threat to other people.
You claim to be a MD. I think you should turn your licence in. Whatever happened to “First do no harm?”
I wonder what conservatives would do if Obama said “You know, it’s really important that everybody breathe.”
I’m guessing we’d find Terry’s body with a plastic bag over his head.
That’s just it. Obama doesnn’t care about anyone drawing breath except himself.
I realize that you get paid to do foodservice work. That isn’t what I asked. I asked if food service workers should have to wash their hands if the boss doesn’t care one way or another. Time wasted on hand washing could be time spent on preparing food. I also asked if there should be laws about the proper handling of food in a restaurant (or slaughterhouse, or bakery, etc.) Nobody pays the restaurant owner to install refrigerators or compensates her for the lost value of potato salad that she has to throw out. Certainly the restaurant owner can rationally decide that the cost of freezers and exterminators and cleaning supplies and wasted food exceeds the cost of insurance to cover potential lawsuits related to food poisoning, and decide to take her chances. Is that OK, or should she be forced to engage in a costly set of behaviors for scarequote public health reasons endscarequote.
It doesn’t matter whether employees lie about having the flu so as to take off work. If a person _is_ sick with an infectious illness, do you think that they have any kind of obligation to stay home from work, and how do you justify it? Missing a shift at work has real economic costs for the employee, and the health of the other employees is not the responsibility of the sick person, is it? Does the sick person have any obligation to stay away from church, or public places, or a friend’s home?
Does a parent have any obligation to keep a kid with chicken pox home from school? The health of other people’s children is not the responsibility of the sick child’s parents, and if the child stays home they lose out on limited educational time and the parents may incur costs. Of course, our wussy nanny state schools may refuse to let the child enter if they find out, but does the parent have any obligation to disclose?
I think we’re all clear on whether you think the government should own the roads. Until the libertarian revolution comes, though, should driving drunk be a crime in the absence of specific damages? Why can the cops throw you in jail just for having a few beers and failing a breath test at a checkpoint? If it’s just because your drivers license represents a contract that you have agreed to – that in return for the privilege of driving you will not do it under the influence, and if so you will be committing a crime – then how will the contracts drafted by the corporations that will control the roads after the glorious libertarian revolution differ? What justification will the corps give for limiting your freedom to knock back a couple of doubles and hit the road?
On the day schools abandon the practice of handing out Perfect Attendance Certificates, and demanding written notes (“Excuse for Absence or Tardiness”) to excuse an absence, your argument will have greater merit.
Just to comment on your claim that “Influenza is the Favorite Malingerer’s Ailment, as bosses everywhere almost universally declare.”
I am surprised to see a physician say this. “Flu” is a term that has a colloquial meaning that’s radically different than its medical meaning. I think you’re calling the common cold influenza. To be fair, people do colloquially refer to it as the flu, including malingerers, I’m sure. But the common cold ≠ influenza. They’re different viruses with different symptoms after onset. Influenza knocks even healthy people out for a week or more with high fever, painful aches, rashes and itching, upper respiratory issues, and fatigue, just to name the common symptoms. It can be deadly to people with compromised or ineffective immune systems like children, the elderly, people who have received transplants, and people with immunodeficiency diseases.
People with influenza aren’t malingering when they don’t go to work. They’re curled up in bed with 103 degree fevers and painful aches that feel like they’re shooting down the center of their bones. I’ve had it. I had to take a bath in cold water to cool my core down because fever reducers couldn’t keep up.
There’s no vaccination for the common cold. There are vaccinations for the strains of influenza whoever is responsible for making these decisions predict will be most common that season. These vaccines are directly responsible for staving off massive outbreaks. Know how we know that? The incidence of influenza infections greatly increases when vaccine producers incorrectly predicted which strains would be prevalent that season.
If you continue to wish to make the claim you did, I refer you to the Spanish flu pandemic of 1918-1919, which killed 50+ million people, or as Wikipedia puts it, 3-5% of the world’s population. There have been several other very deadly outbreaks in the 20th century.
Influenza ain’t no joke, doc.
None of the schools in our school district give out perfect attendance awards. A phone call from a parent giving the reason for an absence is sufficient. Now that that’s out of the way, do parents have any obligation to keep their child out of school when the child is sick? Does an employee have any obligation to stay home when they are sick? Should there be food safety laws for restaurants, etc.? Should drunk driving be a crime absent damages?
I’m trying to determine whether you think an individual should ever feel an obligation – not mandated by external forces – to protect the health of other people at the expense of some loss to themselves. Or if you think there is any justification for making some risky behavior illegal even if no actual injury has occurred.
I grew up in the era of perfect attendance certificates, “Excuses for Absence or Tardiness,” and bosses who bristled at sick calls, saying, “You always have some Delta Alpha Mike November Echo Delta excuse!” So don’t accuse me of making those concepts up out of the whole cloth.
No society stays free while also laying on “prior restraint.” I lived with that principle all my life. I could name dozens of times when I asked for “prior restraint” of a bully, and authorities refused. (That bully, I learned later, wound up stealing a car and going to prison for it.) Now our society has gone to the opposite extreme. We are reaping the wild wind of “prior restraint” with our society that has lost its distinction as the freest on earth.
The only rule that ought to apply is: let the buyer or close associate beware, respect the property and domain of others, and if you break it, you own it. Whether a sick child should attend school anyway, the principal and faculty should decide. Whether an employee should plant his fundament into his cubicle seat, sniffles or no sniffles, his boss should decide. (And the employee should decide whether he wants to work for any given boss, depending on said boss’ policies on communicable diseases, including the common cold, in the workplace.) Whether anyone drives while one might suspect he is impaired, the owner-operator of the road (which, of course, happens to be the government itself, though that wasn’t always the case) has the absolute authority to decide.
Furthermore, any person has the right to explore alternatives to any current artificial immune challenge. Mandating a certain specific preparation, by a specific company or companies, stifles innovation and often “solves” one problem while creating another.
Ok Terry, simple yes or no question: Would you be happy living in a world where smallpox and polio are still a persistent threat?
Also, given your medical expertise, can you explain how Wakefield’s study was even remotely scientific, when it was based on samples from 12 children, obtained under dubious conditions at a birthday party?
Also, given how libertarian’s are always in favour of the “market correcting itself,” how can you continue to defend Wakefied (outside of your need to justify turning children into disease vectors), given that the market corrected itself, declared his work fraudulent and debarred him?
You forfeited your standing to ask the first question, with the very first anti-war comment you posted to this site, and the very first anti-war screed you sent in as a letter to the editor. For that matter, de facto President Obama forfeited his authority to order any sort of quarantine when he made clear he would prefer to live in a world where lawlessness ran rampant, because pax Americana was an ugly, colonialistic thing. So, you just shut up about that.
Now about Dr. Wakefield, I repeat: the so-called re-evaluation of his work was no libertarian market self-correction. It was a travesty of justice, scientific inquiry, and regulatory review. It was a lie, agreed-upon. Did you not catch that the CEO of The Lancet took a position on the Board of Directors of Glaxo SmithKline shortly before Dr. Wakefield’s Kafka-esque “trial” began? There’s your conflict-of-interest. And I thought you liberals hated the drug companies. How quickly you take their side, when they promote the message you write, even when they act like a de facto cartel in so promoting.
“So don’t accuse me of making those concepts up out of the whole cloth.” – Terry
Not sure where the accusation of making stuff up came from. Was it a deleted post?
All I can see MatthewJ saying HIS school district doesn’t have that sort of award and a phone call was sufficient to excuse an absence.
I can add that growing up, my school also did not have attendance awards. So it seems that current practices have changed since “your era” (probably in part for the reason of not incentivizing sick children to come to class).
“On the day schools abandon the practice of handing out Perfect Attendance Certificates,[…] your argument will have greater merit.”
Seems that his argument may have greater merit in many places.
Minor clarification: Stating that a specific school does not currently have attendance awards does not imply that all schools past, present, and future had the same stance.